The StrongMinds breakthrough
Rees Calder · 4 May 2026 · 7 min read
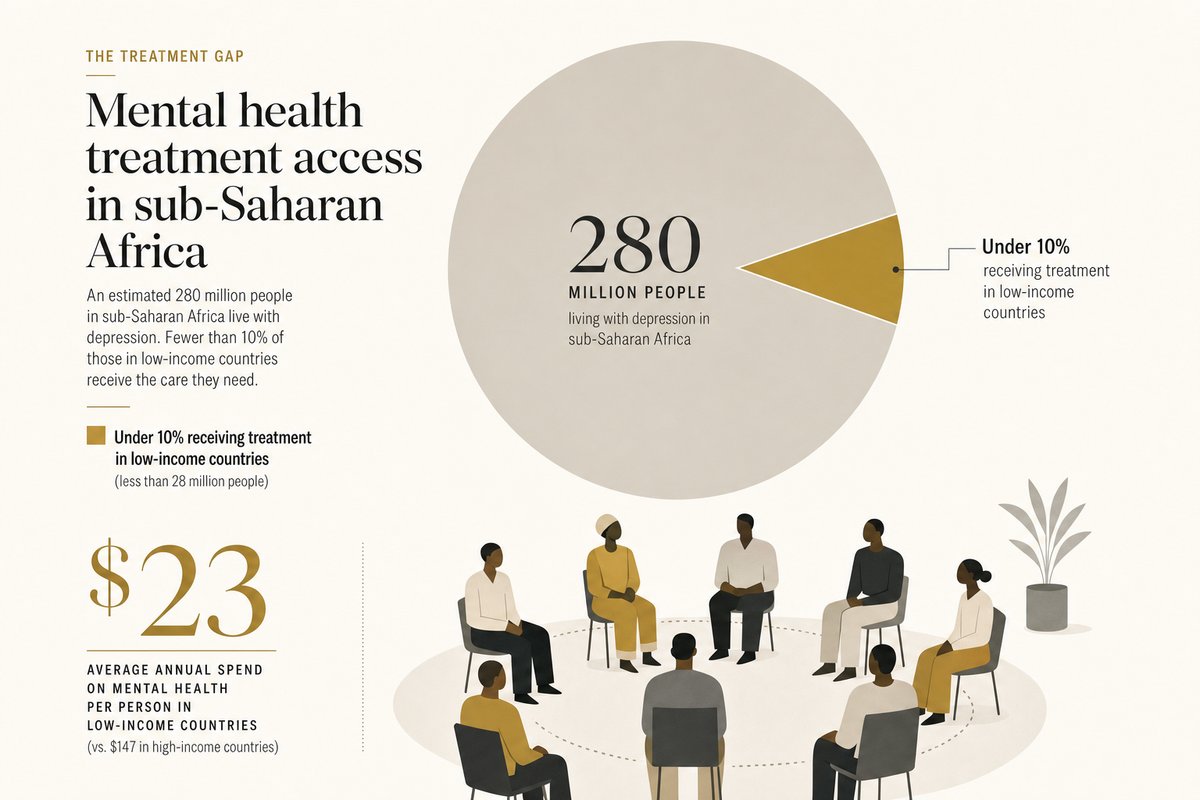
Depression is the leading cause of disability worldwide. The WHO estimates 280 million people suffer from it globally. In sub-Saharan Africa, where mental health services barely exist, fewer than 10% of affected people receive any treatment at all. The workforce numbers explain why: low-income countries have 0.1 psychiatrists and 0.1 psychologists per 100,000 people. Compare that to roughly 15 psychiatrists per 100,000 in the UK.
StrongMinds looked at this gap and asked a different question. Not "how do we train more psychiatrists" (decades, billions, not going to happen soon) but "how do we treat depression without psychiatrists?"
The model: group interpersonal therapy
StrongMinds uses Interpersonal Group Therapy (IPT-G), a form of talk therapy that treats depression by focusing on relationship problems, role transitions, grief, and interpersonal conflict. The WHO recommends IPT-G as the first-line depression intervention in resource-poor settings because it doesn't require clinical psychologists to deliver. Trained lay facilitators can run it.
How it works. Groups of 8-12 people meet weekly for 8-12 sessions. A trained facilitator (often a community health worker, not a clinician) guides the group through structured exercises. Participants identify a specific interpersonal problem connected to their depression, learn communication strategies, practise them with the group, and build a social support network in the process.
The facilitator model. This is the key innovation. StrongMinds trains community-based facilitators who have secondary education but no clinical degree. Training takes weeks, not years. Since 2024, over 1,700 government-paid volunteer facilitators deliver the programme in Uganda and Zambia. The model is designed to integrate into existing public health infrastructure rather than build parallel systems.
Why groups work. Individual therapy is effective but expensive. Group therapy captures roughly 80% of the benefit at a fraction of the cost because the therapist's time serves 8-12 people simultaneously, and the group itself becomes therapeutic. Participants realise their problems aren't unique, practise social skills in real time, and form lasting peer support networks that persist after the programme ends.
The numbers
StrongMinds has treated over 500,000 people for depression since launching in Uganda in 2013 and expanding to Zambia in 2019.
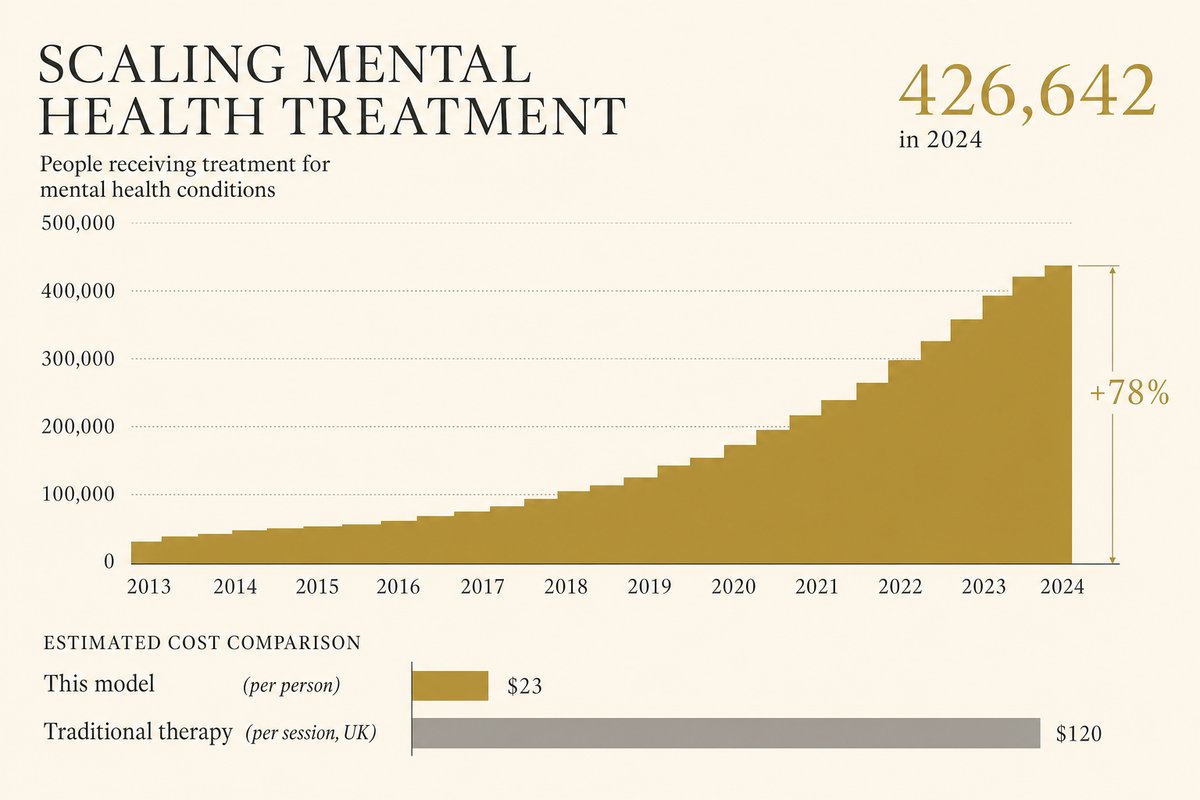
Cost per person: $23. In 2024, StrongMinds drove its cost-per-person treated below its $30 target to just $23. For context, a single therapy session in the UK costs $80-150. StrongMinds delivers an entire 8-12 week programme for less than a third of one session in a high-income country.
2024 scale: 426,642 clients treated. That's a 78% increase over 2023. Of those, 233,185 were treated through government partnerships, meaning the cost was partially borne by national health systems rather than donor funding. That's the scaling pattern: prove it works, train government workers to do it, hand off.
Recovery rate: 71-95%. StrongMinds reports healing rates in this range across programmes, with more than 80% of clients remaining depression-free six months after treatment ends. These aren't self-reported mood improvements. They're measured using validated clinical instruments (the PHQ-9 depression scale).
The cost-effectiveness debate
Do Gooder
One good decision a week
The research behind each piece takes hours. Get the next evidence-backed read every Tuesday, in 3 minutes.
Free weekly read. Unsubscribe anytime, no guilt.
StrongMinds sits at the centre of one of effective altruism's most interesting methodological disagreements: how do you compare preventing depression to preventing death?
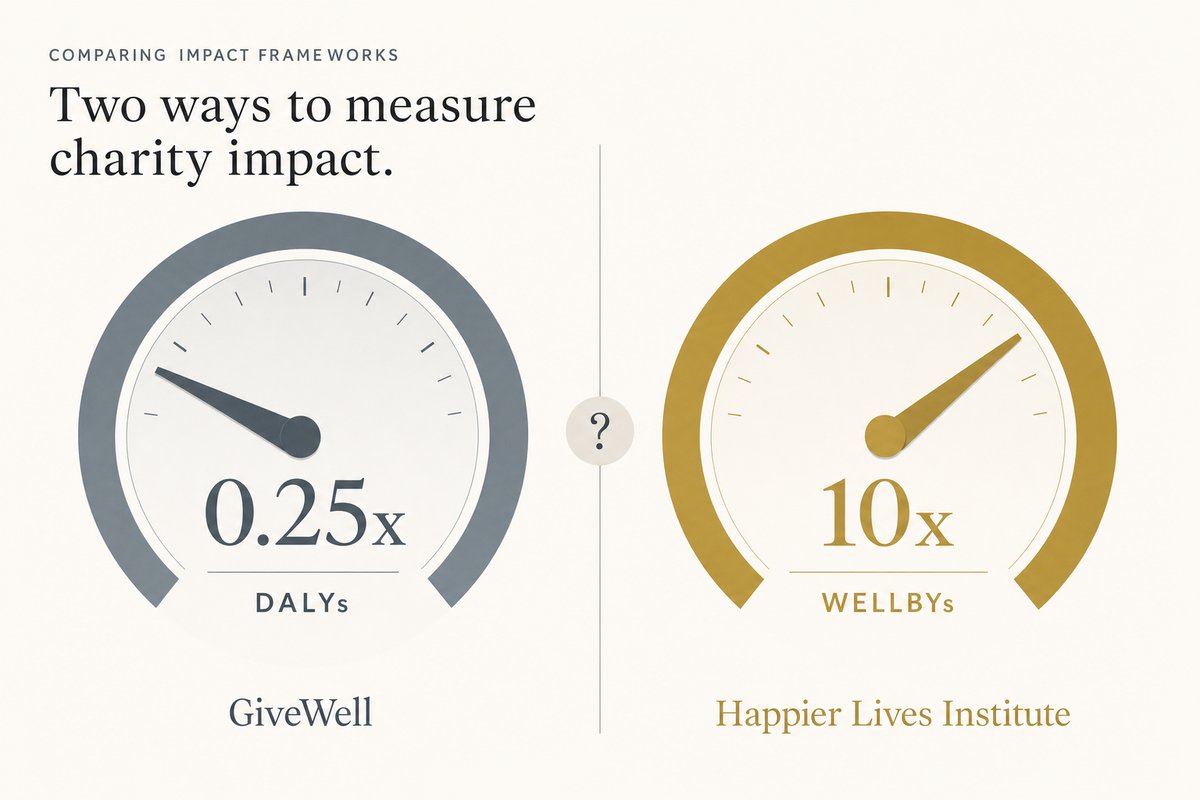
The traditional approach (DALYs). GiveWell evaluates charities using disability-adjusted life years: how many years of healthy life does a dollar buy? Under this framework, GiveWell's best guess puts StrongMinds at roughly 25% as cost-effective as their top-recommended charities (which focus on preventing malaria deaths). Their reasoning: the evidence base for psychotherapy in low-income settings is thinner than for bed nets, the effect sizes are uncertain, and depression may partially resolve without treatment.
The wellbeing approach (WELLBYs). The Happier Lives Institute uses a different metric: wellbeing-adjusted life years. Under this framework, they estimate StrongMinds produces 40 WELLBYs per $1,000, making it roughly 10x more cost-effective than GiveDirectly cash transfers. Their argument: DALYs systematically underweight mental health because they measure disability but not subjective suffering. A year lived with severe depression is rated 0.66 DALYs (meaning it "counts" as 66% of a healthy year), but people experiencing it report wellbeing scores close to zero.
The honest take. The disagreement isn't about StrongMinds specifically. It's about what counts as "doing good." If you think preventing death is categorically different from preventing suffering, DALYs make sense and StrongMinds is decent but not exceptional. If you think a year of severe depression is as bad for the person experiencing it as losing a year of life, WELLBYs make sense and StrongMinds is one of the most cost-effective interventions available.
Founders Pledge, which takes a middle position, estimates StrongMinds at US$377 per DALY averted. That puts it in the range of very good (though not the absolute top of) global health interventions.
Why mental health is neglected
The treatment gap in mental health is staggering even by development standards.
The funding scandal. Depression and anxiety cost the global economy an estimated $1 trillion per year in lost productivity (WHO, 2024). Yet mental health receives roughly 2% of national health budgets in low-income countries, and an even smaller fraction of development aid. Compare this to HIV/AIDS, which receives $540 per person affected versus roughly $0.94 per person affected for mental health conditions.
The workforce impossibility. You cannot solve a problem affecting hundreds of millions of people with 0.1 psychiatrists per 100,000 population. The only viable approach is task-shifting: training non-specialists to deliver evidence-based interventions. This is exactly what StrongMinds does, and exactly why their model matters beyond the people they directly treat. If IPT-G delivered by lay facilitators works at scale (and 500,000 clients suggests it does), it changes the entire calculus of what's possible in global mental health.
The measurement problem. Mental health is harder to count than malaria deaths. You can count bed nets distributed and children who didn't die. Counting depression cases prevented or resolved requires screening tools, follow-up, and willingness to ask people about their inner lives. This measurement difficulty contributes to the funding gap because donors and governments prefer interventions with clear, countable outcomes.
What a donation buys
At $23 per person, the maths are unusually legible for mental health.
- $23: One full course of treatment. One person moves from clinical depression to recovery.
- $230: Ten people treated. Roughly 8 of them will remain depression-free at six months.
- $2,300: One hundred people. A small village's worth of depression eliminated.
- $23,000: One thousand people. The equivalent of StrongMinds' first year of operation, compressed into a single donation.
The ripple effects compound. People who recover from depression return to productive work, parent their children more effectively, and report better physical health. There's evidence that maternal depression treatment improves child development outcomes: when mothers recover, their children's nutrition, school attendance, and emotional regulation all improve.
What to do with this
If you care about the wellbeing framing: StrongMinds may be among the highest-impact donations available. The Happier Lives Institute recommends it as their top charity. A donation here buys large, measurable improvements in subjective wellbeing at very low cost.
If you're more cautious: The evidence base is growing but younger than malaria interventions. GiveWell's concerns about effect size uncertainty are legitimate. A portfolio approach (splitting between StrongMinds and GiveWell top charities) hedges the methodological bet.
Either way: The mental health treatment gap is one of the clearest cases of neglectedness in global health. 280 million people with depression, fewer than 10% treated in the poorest countries, $23 to fix one case. Whatever your moral framework, that ratio demands attention.
More in Bright Spots