The deworming bet
Rees Calder · 25 April 2026 · 7 min read

In 1998, Michael Kremer and Edward Miguel ran a randomised controlled trial in 75 primary schools in Busia district, western Kenya. They gave deworming tablets to children in randomly selected schools and tracked what happened. The results, published in Econometrica in 2004, were striking: school absenteeism dropped by 25%, equivalent to roughly 0.14 additional years of schooling per child treated. The cost per child was under $1 per year.
Those numbers launched one of the most influential, and most contested, interventions in the history of development economics. Two decades later, deworming is still recommended by GiveWell, still funded by hundreds of millions of dollars annually, and still the subject of methodological arguments that illuminate how evidence-based giving actually works in practice.
The original evidence
The Kremer and Miguel study had several features that made it unusually persuasive.
Randomisation at scale. 75 schools, roughly 30,000 children. Not a small pilot. The randomisation was phased: schools were divided into three groups that received treatment in successive years, allowing within-study replication.
Spillover effects. Untreated children in treated schools also showed reduced worm loads, because deworming reduces environmental contamination. This externality means the social return exceeds the private return, strengthening the case for public subsidy.
Cost-effectiveness. At under $1 per child per year for treatment, the cost per year of schooling gained was roughly $3.50. For comparison, other education interventions (textbooks, teacher training, school construction) typically cost $50-200 per additional year of schooling. Deworming was an order of magnitude cheaper.
The study won Kremer the Nobel Prize in Economics in 2019 (shared with Abhijit Banerjee and Esther Duflo), partly for the methodological contribution to development economics and partly for the specific findings on deworming.
The 20-year follow-up
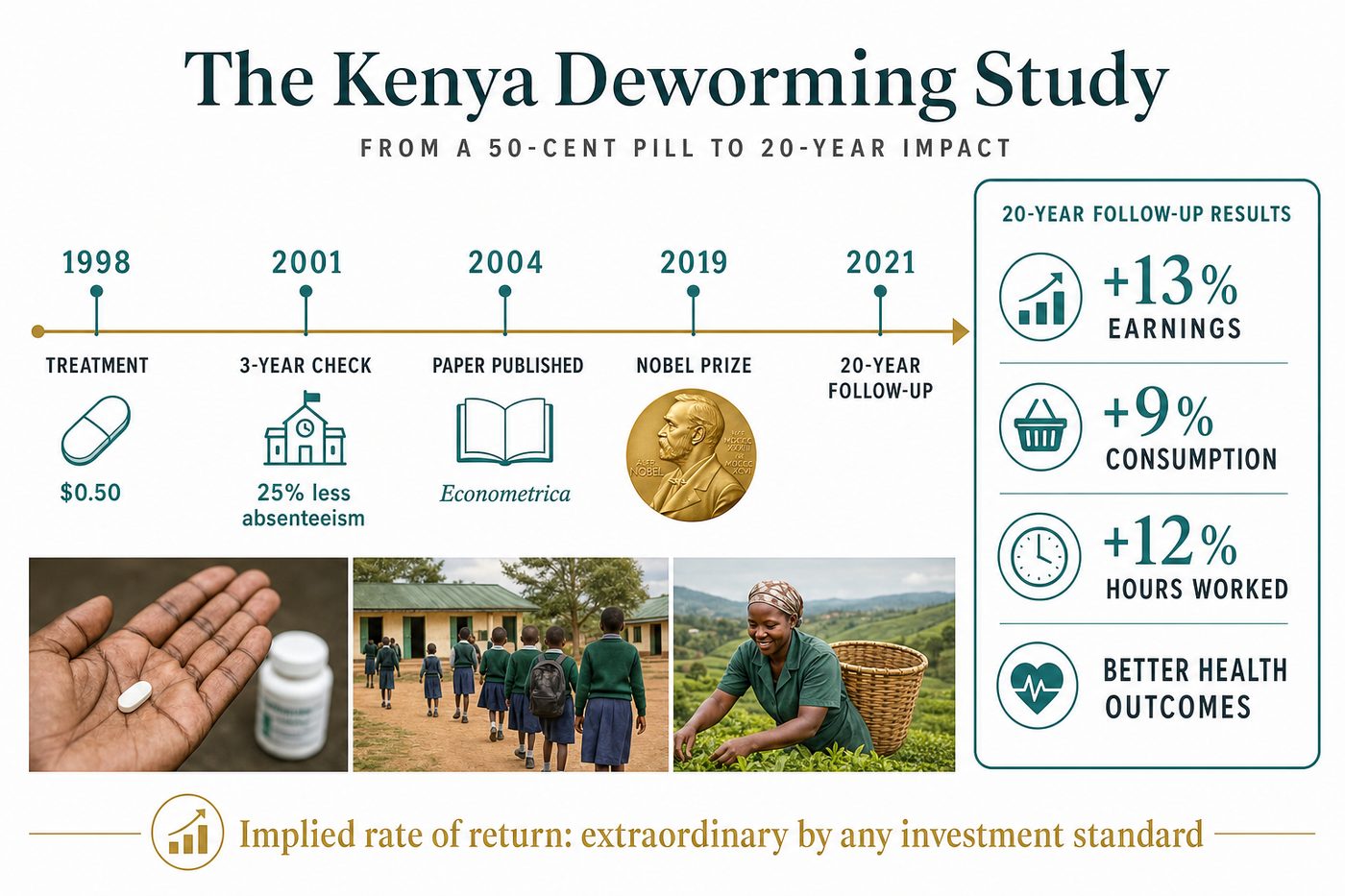
The most remarkable evidence came later. Hamory, Miguel et al. (2021, American Economic Journal: Applied Economics) tracked the original study participants for 20 years. The treated group showed: 13% higher earnings, 9% higher consumption, 12% more hours worked, and measurably better health outcomes in adulthood.
This is extraordinary. A one-time treatment costing less than $1, delivered in childhood, produced measurable economic gains two decades later. The implied rate of return is enormous by any investment standard.
The mechanism: worm infections in childhood cause anaemia, malnutrition, and lethargy that reduce school attendance and cognitive development. Treating them in childhood allows children to accumulate more human capital during the critical developmental window. The gains compound over a lifetime.
The Cochrane controversy
Do Gooder
One good decision a week
The research behind each piece takes hours. Get the next evidence-backed read every Tuesday, in 3 minutes.
Free weekly read. Unsubscribe anytime, no guilt.
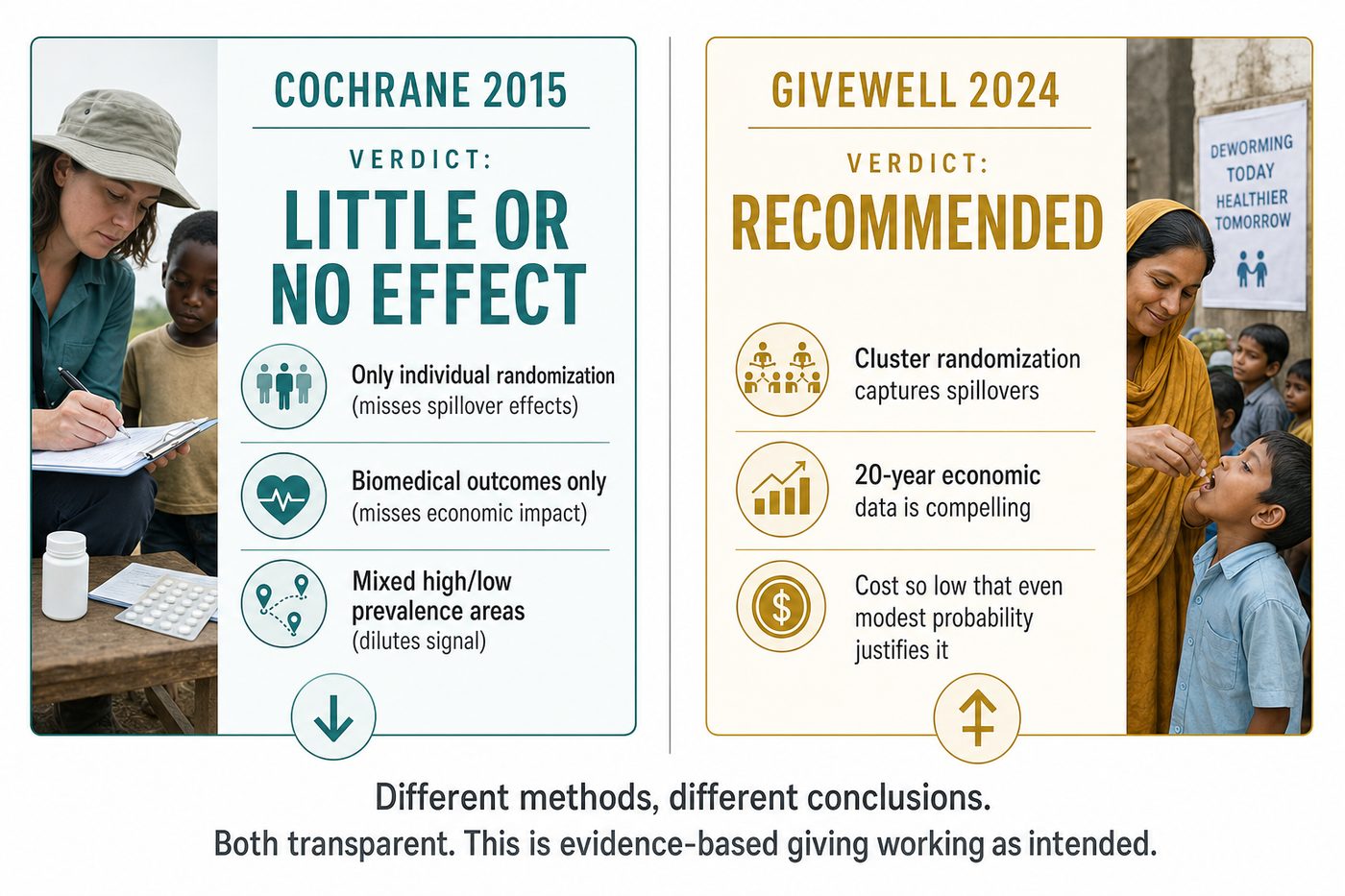
In 2015, the Cochrane Collaboration published an updated systematic review (Taylor-Robinson et al.) that concluded deworming had "little or no effect" on weight gain, haemoglobin, school attendance, or cognition. The headline contradicted the Kremer-Miguel findings directly.
This triggered an intense methodological debate that's worth understanding because it reveals how evidence synthesis can reach opposite conclusions from the same underlying data.
The inclusion criteria. Cochrane included only individually-randomised trials, not cluster-randomised trials like Kremer-Miguel. Since deworming has spillover effects (treating one child reduces infection for nearby children), individual randomisation dilutes the measured effect. The study design that best captures deworming's true impact, cluster randomisation, was excluded by Cochrane's protocol.
The outcome focus. Cochrane focused on biomedical outcomes (haemoglobin, weight) rather than economic outcomes (school attendance, earnings). The biomedical effects of deworming are modest. The economic effects, which operate through school attendance rather than direct health improvement, are large. Different outcome measures, different conclusions.
The context sensitivity. Deworming works in areas with high worm prevalence. Several studies included in the Cochrane review were conducted in areas with low baseline prevalence, where treatment couldn't possibly show large effects. Pooling across high and low prevalence settings dilutes the signal.
GiveWell published a detailed response arguing that the Cochrane methodology was inappropriate for evaluating deworming specifically, and that the long-term follow-up data (which Cochrane didn't consider, as it was published after their review protocol was set) was the most relevant evidence for donors.
Why GiveWell still recommends it
GiveWell's position, updated in their 2024 cost-effectiveness analysis, rests on three pillars.
The long-term evidence is compelling. The 20-year follow-up data is the strongest evidence. Even if the short-term biomedical effects are small, the long-term economic effects are large and consistent across multiple follow-up waves.
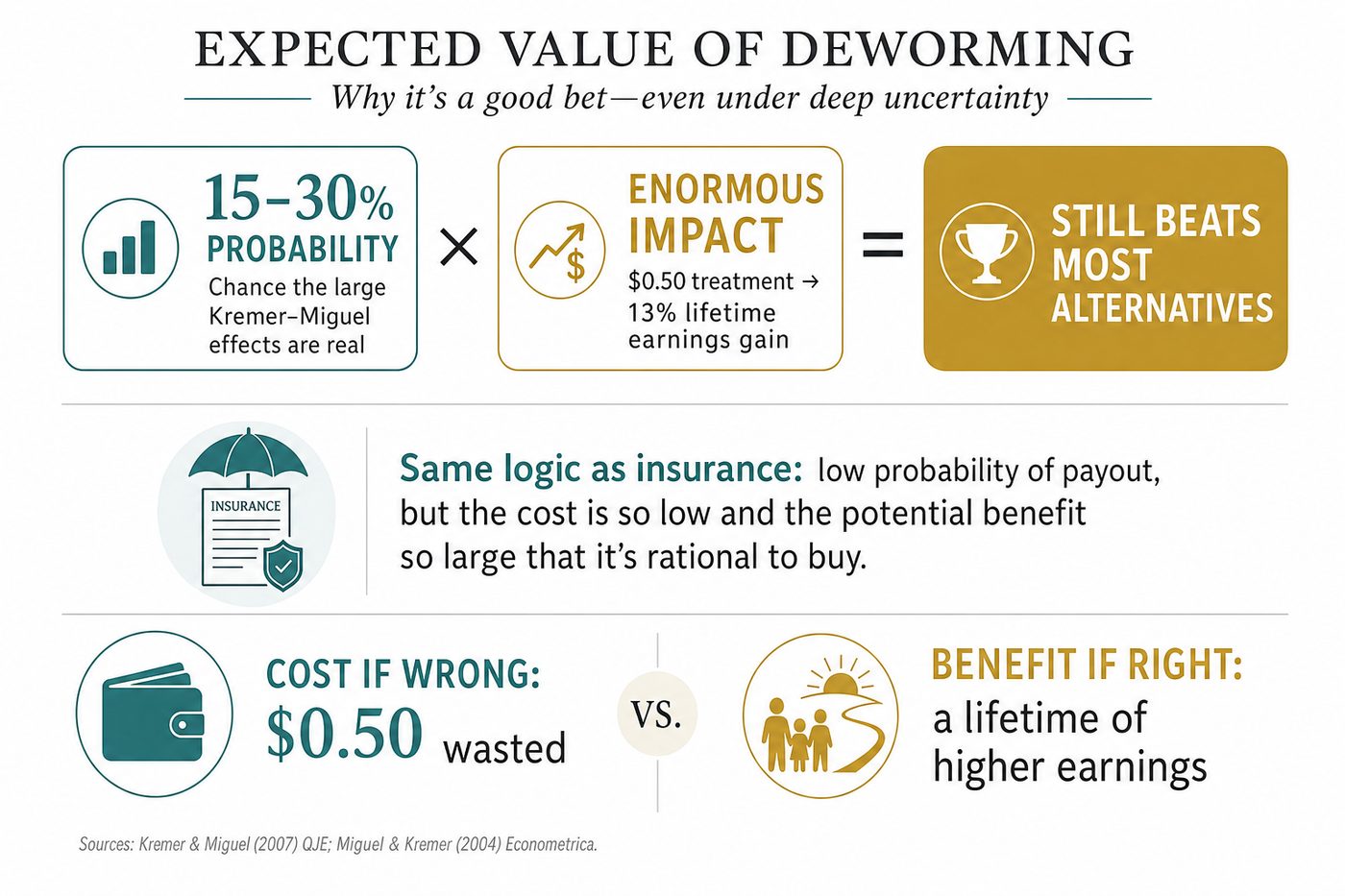
The cost is extraordinarily low. At roughly $0.50-1.00 per child per year, deworming is so cheap that even a small probability of the large effects being real makes it a good bet in expected value terms. GiveWell's model explicitly accounts for uncertainty: they assign roughly 15-30% probability that the Kremer-Miguel effects are approximately correct, and the expected value still exceeds most alternatives.
Scale is proven. Evidence Action's Deworm the World Initiative has treated over 280 million children across India, Kenya, Ethiopia, Nigeria, and other countries. The delivery mechanism (school-based mass drug administration) is simple, cheap, and compatible with existing health infrastructure.
What this teaches about evidence-based giving
The deworming debate illustrates three principles that apply far beyond parasitology.
Expected value thinking beats binary thinking. The question isn't "does deworming work or not?" It's "what's the probability-weighted expected impact per dollar?" When the cost is near zero, even modest probabilities of large effects justify the investment. This is the same logic that makes cheap insurance rational even when the probability of a claim is low.
Long-term follow-ups change the calculus. Most charity evaluation focuses on short-term outcomes because that's what's measurable within a funding cycle. The deworming case shows that the most important effects may only become visible decades later. This argues for funding interventions with plausible long-term mechanisms, even when short-term results are modest.
Methodology debates are inevitable and healthy. The Cochrane-GiveWell disagreement isn't a failure of evidence-based giving. It's evidence-based giving working as intended: different analytical frameworks reaching different conclusions, transparent debate about assumptions, and funders making explicit choices about which evidence to weight. The alternative, giving based on anecdote and emotion, doesn't produce this kind of productive disagreement.
For your giving
Deworming is a reasonable high-expected-value bet for donors who accept GiveWell's framework. If you want to fund it specifically, Evidence Action's Deworm the World Initiative is GiveWell's recommended vehicle. SCI Foundation (now SCI, the Schistosomiasis Control Initiative at Imperial College London) is another established deworming charity.
If the uncertainty bothers you, GiveWell's "Maximum Impact Fund" allocates across their top recommendations including deworming, letting you diversify across their highest-confidence interventions.
The honest framing: this is a bet, not a certainty. But it's a well-reasoned bet with a favourable expected value, and the downside (spending $0.50 on a tablet that might not help much) is about as low as charity downsides get.
One sentence
Deworming is the cheapest bet in effective giving: under $1 per child, contested short-term evidence, spectacular long-term data, and a cost so low that the expected value calculation favours it even under deep uncertainty.
Sources used: Kremer and Miguel "Worms: Identifying Impacts on Education and Health in the Presence of Treatment Externalities" (Econometrica, 2004), Hamory, Miguel et al. "Twenty-Year Economic Impacts of Deworming" (American Economic Journal: Applied Economics, 2021), Taylor-Robinson et al. "Deworming drugs for soil-transmitted intestinal worms in children" (Cochrane Database of Systematic Reviews, 2019 update), GiveWell deworming cost-effectiveness analysis and Cochrane response (2024), Evidence Action Deworm the World programme data (2024), Nobel Prize Committee citation for Kremer, Banerjee, Duflo (2019). Full links in the planning doc.
More in Bright Spots