The Against Malaria Foundation
Rees Calder · 25 April 2026 · 7 min read

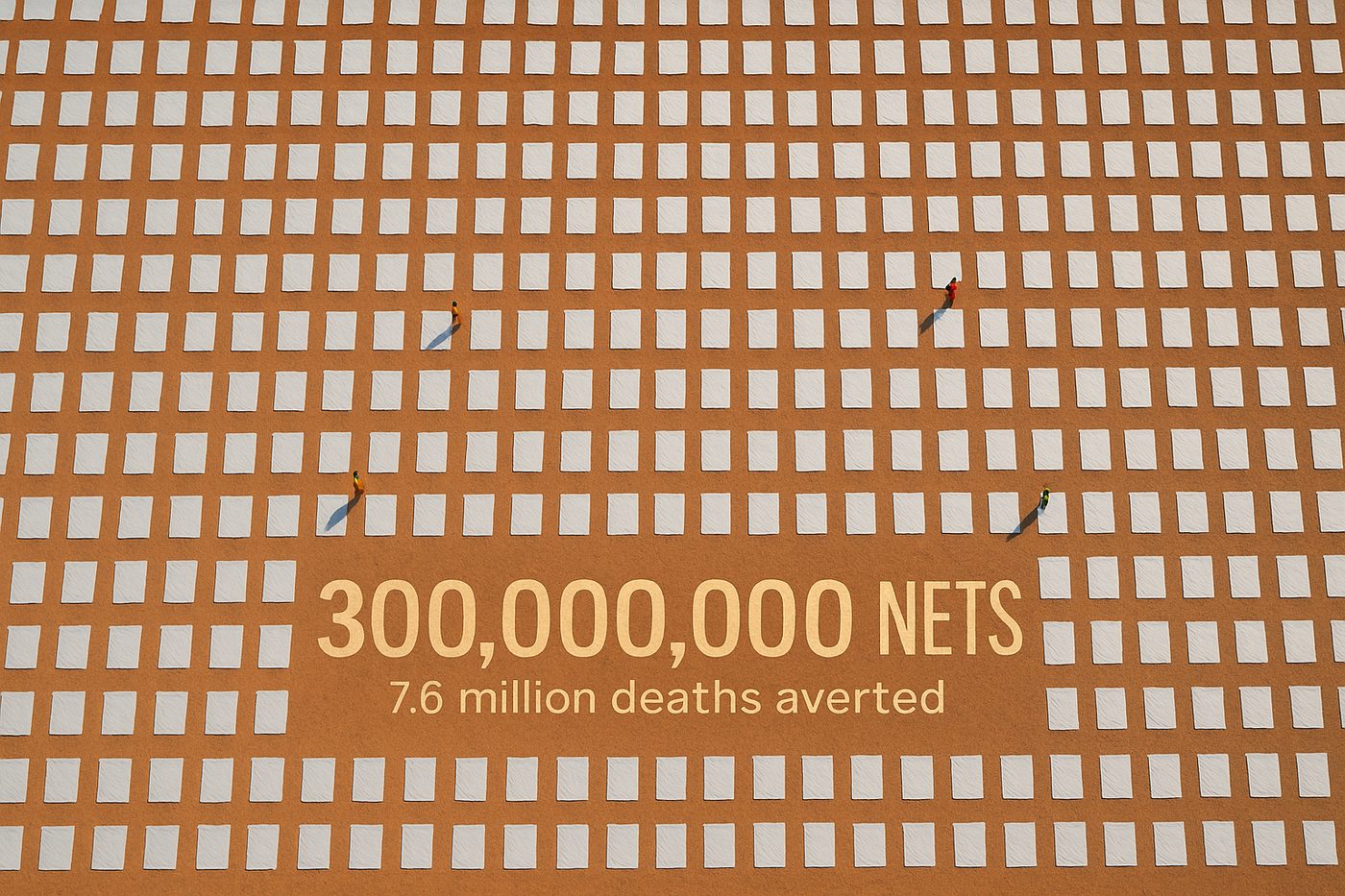
Rob Mather started the Against Malaria Foundation in 2004 after watching a documentary about children dying from malaria. Twenty years later, AMF has distributed over 300 million insecticide-treated bed nets across sub-Saharan Africa, and has been GiveWell's top or near-top recommended charity for more than a decade running. It's the closest thing the effective giving world has to a consensus answer to "where should I donate?"
The reason is not charisma or marketing. AMF barely markets at all. The reason is evidence, cost-effectiveness, and a relentless focus on doing one thing well.
The intervention
Long-lasting insecticide-treated nets (LLINs) prevent malaria by creating a physical and chemical barrier between sleeping humans and the Anopheles mosquitoes that carry the Plasmodium parasite. The nets are treated with pyrethroid insecticides that both repel and kill mosquitoes on contact.
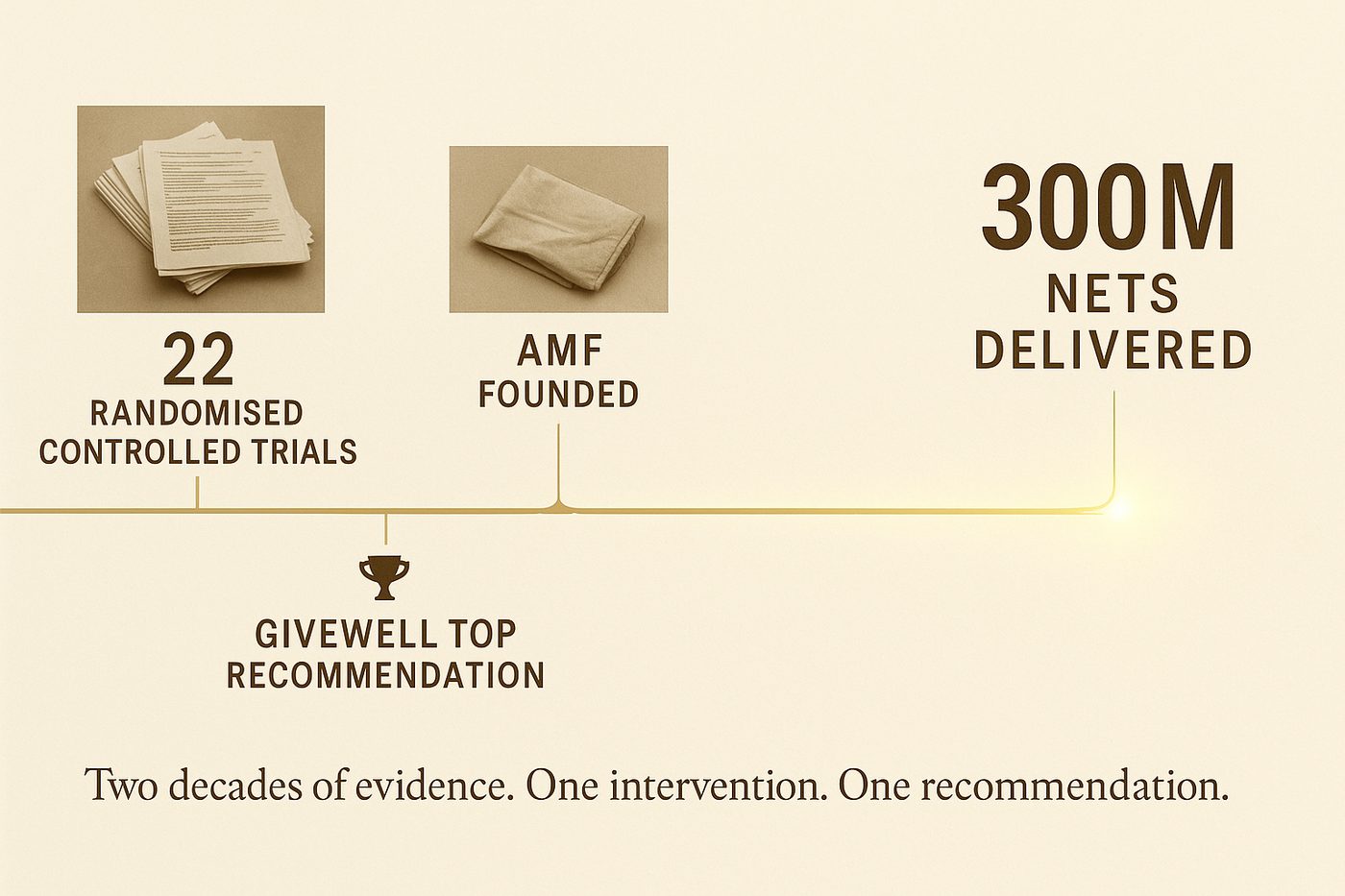
The evidence base is unusually strong. A 2004 Cochrane systematic review by Lengeler, covering 22 randomised controlled trials across multiple African countries, found that ITNs reduce all-cause child mortality by roughly 17% in areas with stable malaria transmission. A 2018 update by Pryce, Richardson and Lengeler confirmed the finding with additional data. No other single public health intervention achieves comparable mortality reduction at comparable cost in malaria-endemic regions.
The WHO estimates that bed nets have averted roughly 1.5 billion malaria cases and 7.6 million deaths since 2000 (World Malaria Report, 2023). Not all of those nets came from AMF, obviously. But AMF's contribution of 300 million+ nets makes it one of the largest non-governmental distributors.
The cost-effectiveness case
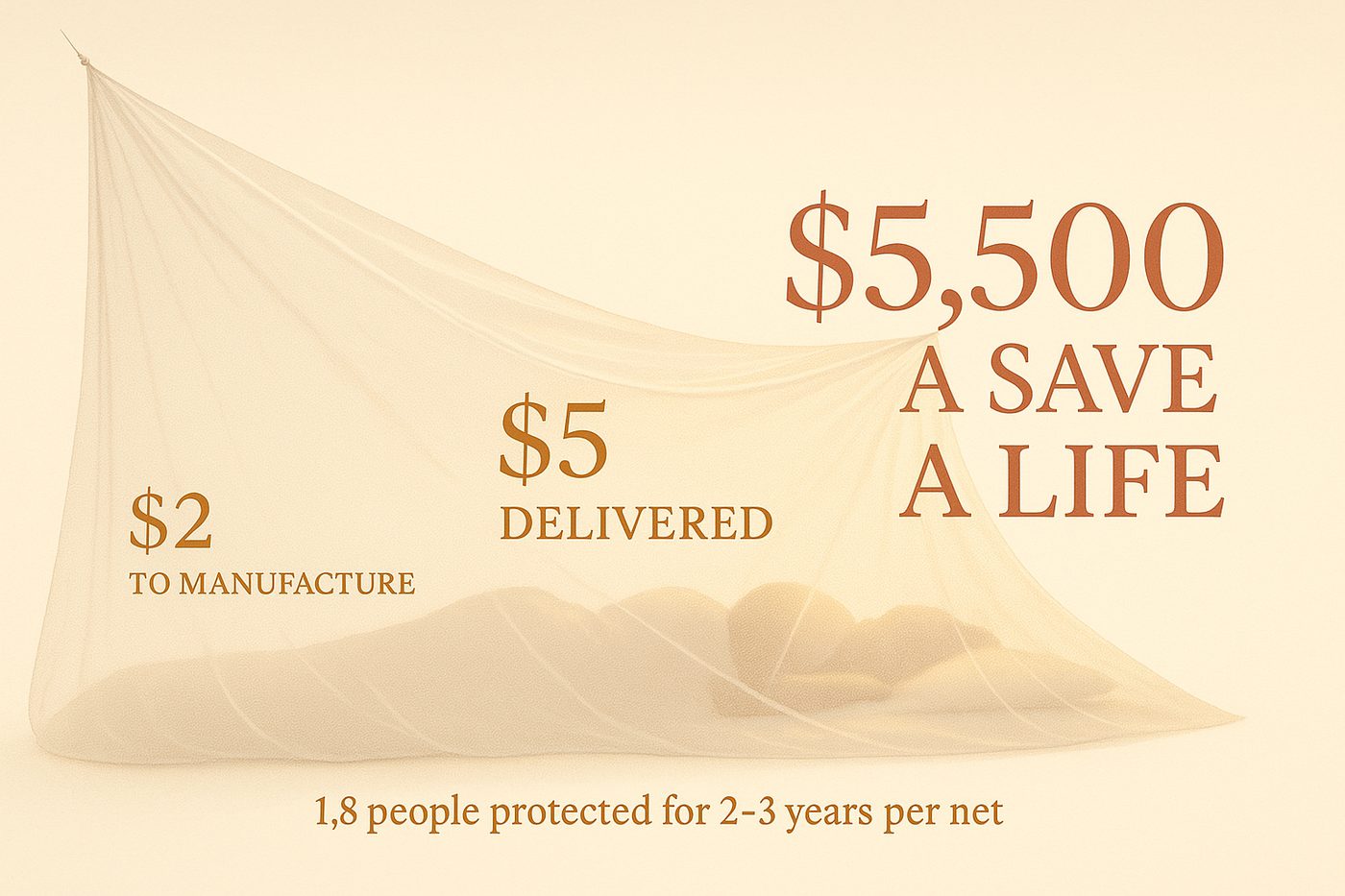
GiveWell's 2024 cost-effectiveness model estimates that AMF saves a life for roughly 5,500 dollars (with significant uncertainty: the 90% confidence interval runs from approximately 3,000 to 12,000 dollars). In terms of cost per disability-adjusted life year (DALY) averted, the figure is roughly 50 to 100 dollars.
For context: the World Health Organization's traditional threshold for a "very cost-effective" health intervention is one that costs less than the GDP per capita of the country in question per DALY averted. In the DRC (GDP per capita roughly 580 dollars), AMF's cost per DALY is roughly 10-15% of that threshold. By any standard measure, it's extraordinarily cost-effective.
Three factors drive this.
Low unit cost. A single LLIN costs roughly 2 to 3 dollars to manufacture and 50 cents to a dollar to distribute. The total cost per net delivered, including all overheads, is roughly 4 to 5 dollars. Each net protects an average of 1.8 people for 2-3 years.
High disease burden. Malaria kills roughly 600,000 people per year (WHO, 2023), the vast majority children under five in sub-Saharan Africa. The sheer scale of the problem means that even a modest reduction in transmission rates saves a large number of lives in absolute terms.
Strong implementation. AMF's distribution model involves partnerships with national malaria control programmes, pre-distribution registration surveys (to size the need accurately), post-distribution check-ups at 6, 12, 24, and 36 months (to verify nets are hung and in use), and public data transparency. The post-distribution monitoring is what distinguishes AMF from many other net distributors: they actually verify that nets reach households and get used.
What makes AMF unusual
Do Gooder
One good decision a week
The research behind each piece takes hours. Get the next evidence-backed read every Tuesday, in 3 minutes.
Free weekly read. Unsubscribe anytime, no guilt.
Three organisational features worth noting.
Radical transparency. AMF publishes every distribution agreement, every survey dataset, every monitoring report on their website. You can see exactly which nets went where, when, and what the follow-up data showed. This level of transparency is almost unheard of in the charity sector. GiveWell has cited it repeatedly as a factor in their recommendation.

Minimal overhead. AMF operates with a staff of roughly 10 people. Rob Mather, the founder and CEO, has worked unpaid for the organisation's entire history. Total overhead is roughly 3-5% of funds raised. This matters not because overhead ratios are a good metric for charity quality (they're not, as explored in "The overhead myth"), but because it means nearly all donated funds convert to nets.
Single intervention focus. AMF does one thing: fund bed nets. They don't run health clinics, train community health workers, or advocate for policy change. The advantage: every part of the organisation is optimised for one outcome. The disadvantage: they can't address the broader malaria effort (treatment, diagnostics, vaccine rollout, insecticide resistance). They've made a deliberate tradeoff, and the evidence suggests it's the right one for a donation-funded charity.
The criticisms, honestly
Insecticide resistance. Pyrethroid resistance in Anopheles mosquitoes has been rising across sub-Saharan Africa since the mid-2010s. The Lancet published data in 2022 showing that resistance prevalence exceeds 50% in many regions. This threatens the effectiveness of standard LLINs. AMF has responded by shifting toward next-generation nets treated with multiple insecticides (piperonyl butoxide synergist nets and dual-AI nets), which maintain efficacy against resistant mosquitoes but cost roughly 50% more per net.
Marginal impact uncertainty. As net coverage has increased (reaching roughly 68% of at-risk populations per the WHO's 2023 data), the marginal impact of each additional net likely decreases. GiveWell's model accounts for this with a diminishing returns curve, but the precise shape of that curve is uncertain. AMF may be somewhat less cost-effective today than it was in 2010, when coverage was lower.
Vaccine competition. The RTS,S malaria vaccine (Mosquirix), approved by WHO in 2021, and the more effective R21/Matrix-M vaccine, approved in 2023, may change the cost-effectiveness calculus. If vaccine rollout accelerates, the marginal value of nets could decline further. However, current projections suggest vaccine and net programmes are complements, not substitutes: the WHO recommends both.
What it teaches about giving
AMF illustrates four principles that apply beyond malaria.
Specificity wins. A charity that does one thing well is easier to evaluate, easier to fund, and often more effective than one that does many things adequately.
Evidence compounds. AMF has benefited from two decades of accumulating data. Each distribution generates monitoring data that improves the next distribution. The learning curve is real and measurable.
Transparency is a competitive advantage. AMF's openness has earned it sustained support from GiveWell, which has directed hundreds of millions of dollars in donations. Transparency isn't just ethical. It's strategic.
Scale doesn't require bureaucracy. 300 million nets, 10 staff. The model works because AMF partners with existing national programmes rather than building parallel infrastructure.
One sentence
AMF has saved hundreds of thousands of lives by doing one thing, distributing bed nets, with extraordinary cost-effectiveness, radical transparency, and a two-decade evidence base that keeps getting stronger.
Sources used: GiveWell AMF cost-effectiveness analysis (2024), Against Malaria Foundation distribution data and monitoring reports (2024), WHO World Malaria Report (2023), Lengeler "Insecticide-treated bed nets and curtains for preventing malaria" (Cochrane Database of Systematic Reviews, 2004, updated Pryce et al. 2018), Lancet insecticide resistance data (2022), WHO RTS,S and R21 vaccine recommendations (2021, 2023). Full links in the planning doc.
More in Bright Spots