The biosecurity bet
Rees Calder · 6 May 2026 · 7 min read
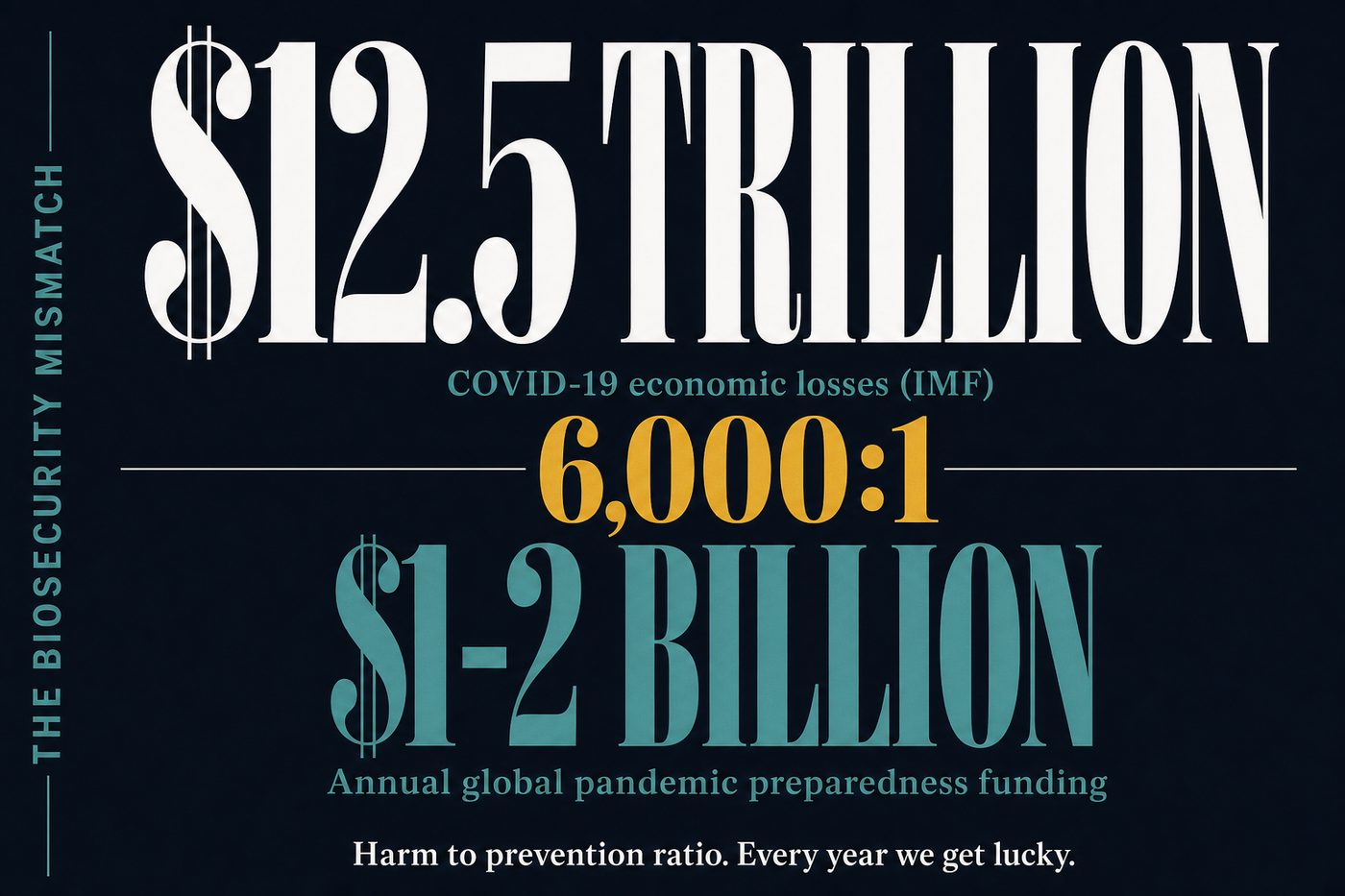
COVID-19 cost the world approximately $12.5 trillion in direct economic losses, according to the IMF. About 7 million people died officially. Excess death estimates put the real figure closer to 15-20 million. The pandemic wiped out a decade of poverty reduction progress in the span of two years.
Philanthropic funding for pandemic preparedness globally runs at about $1-2 billion per year.
That ratio, somewhere between 6,000:1 and 12,000:1 in harm versus prevention spending, is what the effective philanthropy community calls a "neglected cause." It is, by any honest accounting, one of the stranger failures of collective human attention.
What the money actually buys
Pandemic preparedness isn't one thing. The field has distinct layers, and the philanthropic leverage varies dramatically between them.
Surveillance infrastructure. Most pandemic response failures start the same way: a novel pathogen spreads for weeks or months before anyone identifies and reports it. The gap between a virus emerging and a government issuing a public health alert can be measured in deaths averted. Organisations like the Global Health Security Index track which countries have functional early warning systems. In most of Africa, South Asia, and parts of Latin America, the answer is: not really.
CEPI (the Coalition for Epidemic Preparedness Innovations) allocates a portion of its budget here, as does the Wellcome Trust. The marginal cost of improving surveillance in a high-risk spillover zone (dense human-animal interaction, low testing capacity, weak public health infrastructure) is low. The expected benefit is enormous and hard to quantify, which is partly why this work is underfunded. It's hard to fundraise for a catastrophe that didn't happen.
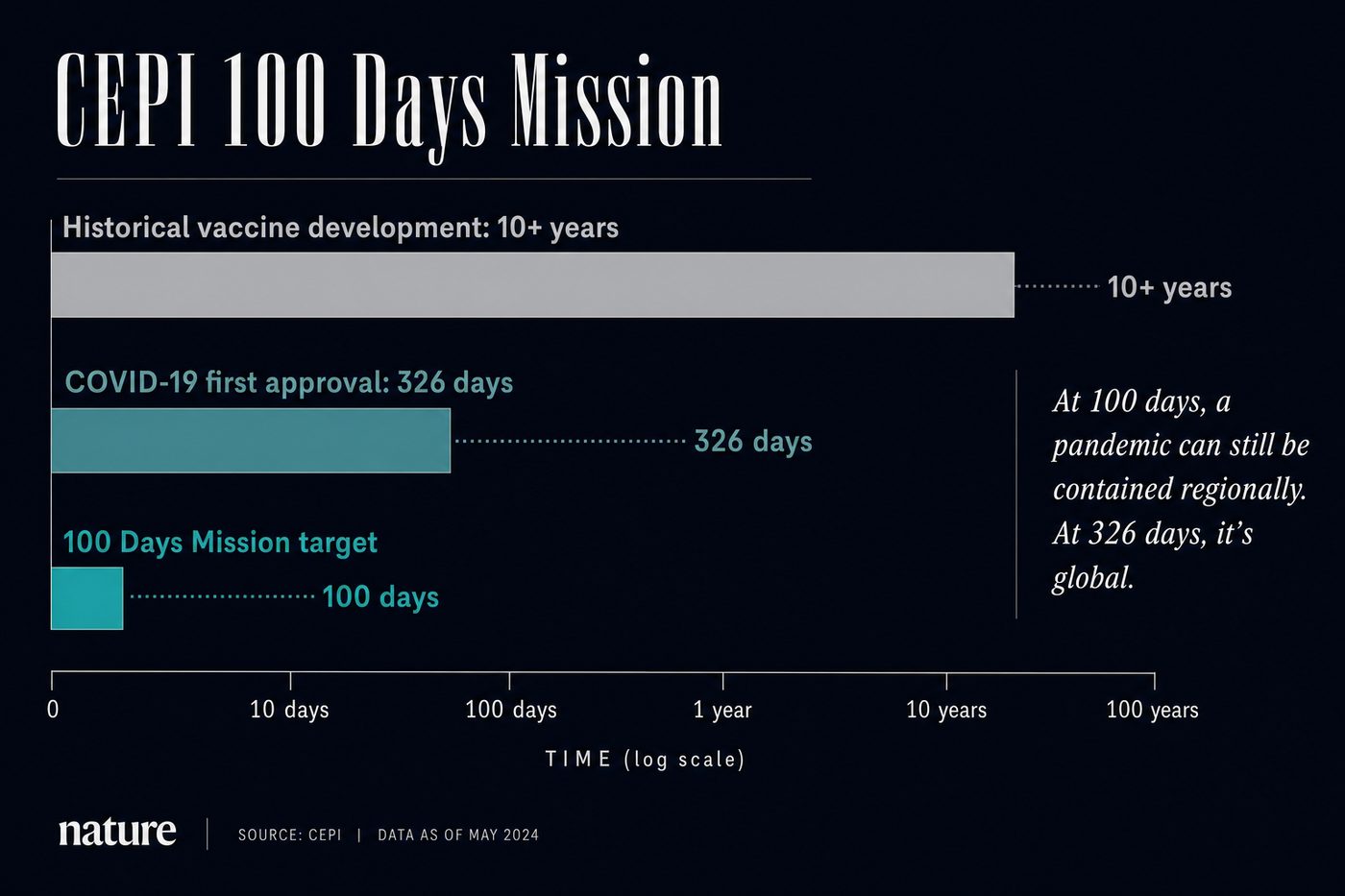
Vaccine platform development. CEPI's headline mission is reducing the time from pathogen identification to a deployed vaccine from the historical 10+ years to 100 days. They came close with COVID (about 326 days for the first regulatory approval). The 100 Days Mission is technically ambitious but the target isn't arbitrary: in a fast-spreading respiratory pandemic, 100 days versus 300 days likely determines whether the thing stays regional or goes global.
CEPI raised about $1.5 billion in pledges as of 2024 and estimates it needs $3.5 billion for its next five-year plan. That funding gap is real and specific.
Policy and international coordination. The WHO's pandemic treaty negotiations have dragged for years. National health ministries have short time horizons and respond to visible crises, not statistical expectations. Organisations like the Nuclear Threat Initiative's biosecurity program and the Johns Hopkins Center for Health Security (now folded into the Bloomberg School of Public Health after funding cuts in 2024) do the slow, thankless work of building policy infrastructure that makes global coordination possible when a pathogen actually emerges.
This is unglamorous, hard to evaluate, and genuinely important. Private philanthropy can sustain it in ways that government funding cannot, because it requires continuity across election cycles.
Why the effective philanthropy community pays attention
There's a standard framework for assessing whether a cause area deserves more funding: scale, neglectedness, and tractability. Pandemic preparedness scores unusually well on all three.
On scale: pathogens are one of very few risks capable of killing millions in a short time frame. Beyond the death toll, the economic and social disruption is civilisation-scale. This isn't speculation. It's the observed record, from 1918 to 2020.
On neglectedness: global health philanthropy is heavily concentrated in HIV/AIDS, malaria, tuberculosis, and maternal health. These are important and relatively well-served. Pandemic preparedness competes for attention and funding and usually loses, because prevention is invisible and treatment is legible.
On tractability: we know what the interventions are. Surveillance infrastructure, vaccine platform technology, international coordination frameworks, stockpile management. These aren't research questions. They're funding and execution problems.
Open Philanthropy, the largest EA-adjacent funder, has committed roughly $300-400 million to biosecurity over several years. That's large in absolute terms and a rounding error against the expected losses from the next pandemic.
Who is doing the work
Do Gooder
One good decision a week
The research behind each piece takes hours. Get the next evidence-backed read every Tuesday, in 3 minutes.
Free weekly read. Unsubscribe anytime, no guilt.
The field is smaller than it should be, which at least makes it easier to map.
CEPI is the most directly fundable via public giving. It accepts donations and is one of the few organisations in this space with a legible theory of change and measurable deliverables.
Resolve to Save Lives (founded by Tom Frieden, former CDC director) works on epidemic preparedness in lower-income countries. Funded partly by Bloomberg Philanthropies and Open Philanthropy.
NTI Biosecurity (Nuclear Threat Initiative) focuses on the policy and governance layer: biosecurity indices, treaty frameworks, laboratory safety standards. Not directly fundable by most donors but produces the research that shapes what governments actually do.
Johns Hopkins Bloomberg School of Public Health absorbed the Center for Health Security in 2024. Losing the CHS as a standalone entity with its own brand was a setback. The work continues but with less visibility.
Wellcome Trust is the largest private funder in global health and has pandemic preparedness as an explicit priority. Not fundable by individuals but worth tracking for the state of the field.
The honest caveats
Biosecurity philanthropy is harder to evaluate than bednet distribution or vitamin A supplementation. The counterfactuals are invisible by design: if the next pandemic is contained to a few thousand cases because surveillance caught it early, nobody will write about the 10 million people who didn't die. The field runs on expected value reasoning, which is correct but uncomfortable.
There's also genuine scientific uncertainty about what the next pandemic looks like. Respiratory RNA viruses are the historical worry (influenza, coronaviruses). Engineered pathogens are a newer and harder-to-model concern. The interventions that help with natural pandemic risk also help with engineered risk, but not symmetrically.
For donors who want something measurable within their own lifetimes, pandemic preparedness is a harder psychological fit than GiveWell's top charities. You're betting on the absence of a catastrophe, and wins in this space don't feel like wins.
What to do with this
If pandemic preparedness fits your risk tolerance and worldview, CEPI is the most direct giving vehicle for individuals. Founders Pledge has done detailed analysis of the cause area and recommends CEPI and Wellcome Leap as the most cost-effective options for donor giving.
If you want to stay informed without giving: Johns Hopkins Bloomberg School, Resolve to Save Lives, and the NTI biosecurity program all publish accessible research. The Global Health Security Index tracks country-by-country preparedness every two years, and it's grimly readable.
The field needs more funders. The expected value of being one of them is hard to overstate and easy to ignore, right up until it isn't.
Sources used
- IMF World Economic Outlook: COVID-19 economic impact estimates ($12.5T, 2021-2022 data)
- CEPI 100 Days Mission: technical targets, funding gap ($3.5B five-year plan)
- Open Philanthropy biosecurity grant portfolio (public grant database)
- Global Health Security Index 2023 (Johns Hopkins Bloomberg School / NTI)
- Founders Pledge "Pandemic Preparedness" cause report (2021, updated 2023)
- Resolve to Save Lives annual reports
- WHO excess mortality estimates COVID-19 (2022, updated 2024)
- Nuclear Threat Initiative Biosecurity program overview
More in The Map