The cost per outcome
Rees Calder · 27 April 2026 · 7 min read
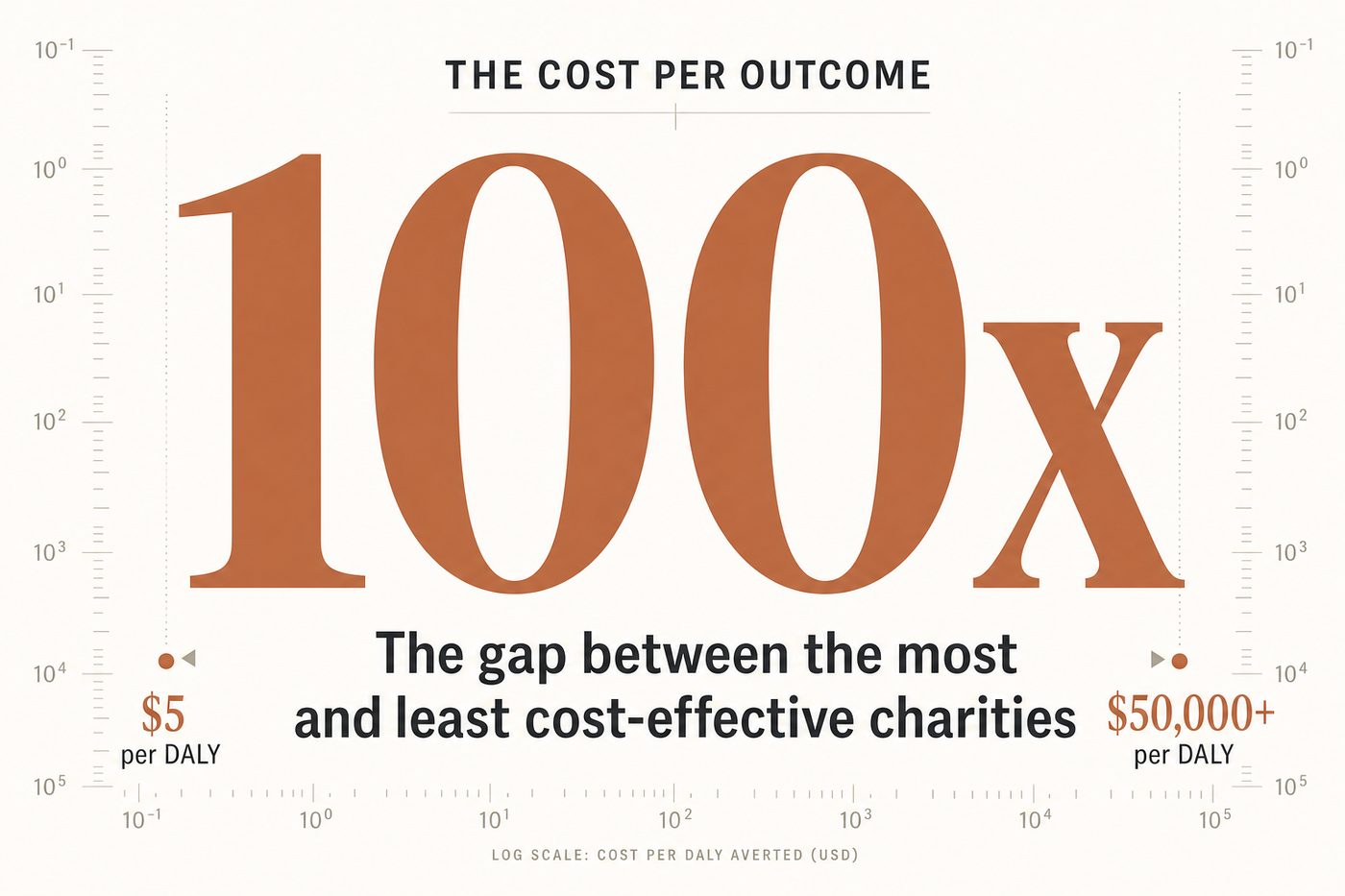
Here's a number that should change how you think about charity. The most cost-effective health interventions in the world are roughly 100 times more effective per dollar than the median intervention for the same problem. Not 2x. Not 10x. One hundred times.
That kind of gap comes out of the cost-effectiveness data in the Disease Control Priorities project (published by the World Bank), which systematically estimated the cost per disability-adjusted life year (DALY) averted for hundreds of health interventions across low and middle-income countries. The cheapest interventions cost roughly $3-10 per DALY averted (childhood vaccination, deworming, oral rehydration therapy). The most expensive run into the tens of thousands of dollars per DALY (some surgical oncology, certain chronic disease management). Analysing the DCP2 data, Toby Ord found that the most cost-effective intervention was about 60 times more cost-effective than the median and roughly 15,000 times the least effective. The "roughly 100x better than the median" framing used across the effective giving community sits in that range once you also account for differences in how well organisations deliver an intervention.
For donors, this means the choice of where to give matters far more than the choice of how much. Giving £1,000 to a top-tier charity can produce the same outcome as giving £100,000 to a median one. No other decision in personal finance has this kind of leverage.
What "cost per outcome" means
Three metrics dominate the cost-effectiveness field. Worth knowing the differences.
Cost per DALY averted. A DALY (disability-adjusted life year) combines years of life lost to premature death with years lived with disability into a single measure. One DALY averted equals one year of full health gained. The WHO and World Bank use DALYs as the standard currency for comparing health interventions. Lower cost per DALY = more health per pound.
Cost per life saved. Simpler and more intuitive but less precise. GiveWell uses cost per life saved (or per death averted) as a headline metric for top charity recommendations. Their estimates put it at roughly $2,000-$7,000 per death averted for the Malaria Consortium's SMC programme and in the same broad range, around $4,500-$5,500 on average, for the Against Malaria Foundation, varying by location (GiveWell, "How Much Does It Cost to Save a Life," 2024 version).
Cost per unit of welfare. The broadest measure, used by GiveWell in their newer "moral weights" framework. Attempts to compare across different types of outcomes: how much is a year of schooling worth relative to a year of health? How do you compare averting a death to increasing income by 13% for 20 years? This gets philosophical fast, and GiveWell publishes their assumptions explicitly so donors can adjust.
The 100x gap in practice
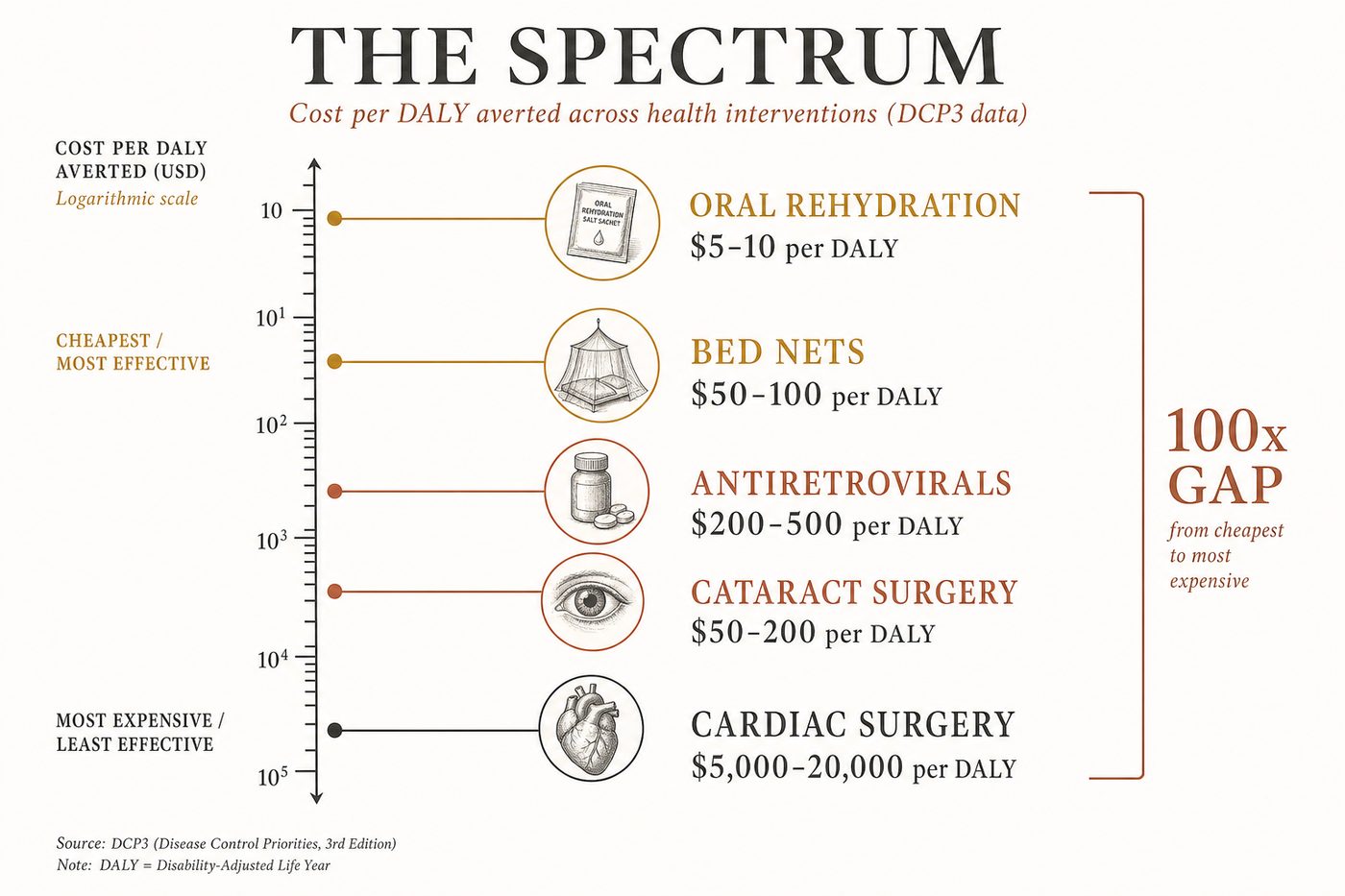
Five examples across the cost-effectiveness spectrum, from DCP3 and GiveWell data.
Oral rehydration therapy for childhood diarrhoea. Cost per DALY averted: roughly $5-10. A packet of oral rehydration salts costs less than $0.50 and prevents death from dehydration. This is among the most cost-effective health interventions ever identified. It's been available since the 1970s and is estimated to have saved on the order of 50 to 70 million lives, mostly children (Our World in Data).
Insecticide-treated bed nets. Cost per DALY averted: roughly $50-100 (GiveWell, 2024). A net costs $4-5 delivered, protects 1.8 people for 2-3 years, and reduces malaria mortality by roughly 17%. Extraordinarily cost-effective by any standard.
Antiretroviral therapy for HIV. Cost per DALY averted: roughly $200-500 in sub-Saharan Africa (DCP3). A genuine medical miracle, but roughly 5-10x more expensive per DALY than the cheapest interventions. Still highly cost-effective by WHO thresholds.
Cataract surgery. Cost per DALY averted: roughly $50-200 depending on setting (DCP3). Restores sight for roughly $50-100 per surgery in low-income countries. One of the most cost-effective surgical interventions.
Cardiac surgery in low-income settings. Cost per DALY averted: roughly $5,000-20,000 (DCP3). Genuinely lifesaving, but 100-1000x less cost-effective per DALY than oral rehydration or deworming. This doesn't mean it's not worth doing. It means that a donor optimising for health impact per pound should fund it only after cheaper interventions are fully funded.
Why the gap exists
Do Gooder
One good decision a week
The research behind each piece takes hours. Get the next evidence-backed read every Tuesday, in 3 minutes.
Free weekly read. Unsubscribe anytime, no guilt.
Three reasons the cost-effectiveness range is so wide.
Technology costs vary enormously. A packet of ORS costs pennies. An operating theatre costs millions. The underlying technology determines the floor on cost per outcome, and that floor varies by orders of magnitude across interventions.
Diminishing returns within interventions. The first million bed nets distributed in a region with zero coverage produce much more health gain per net than the last million in a region at 80% coverage. Cost-effectiveness estimates are marginal: they measure what the next pound achieves, not the average of all pounds ever spent. As coverage increases, cost-effectiveness decreases.
Implementation efficiency varies. Two organisations delivering the same intervention can differ 3-5x in cost-effectiveness based on operational efficiency, overhead, targeting accuracy, and scale. This is why GiveWell evaluates organisations, not just interventions: the delivery matters as much as the medicine.
What this means for donors
Four practical implications.
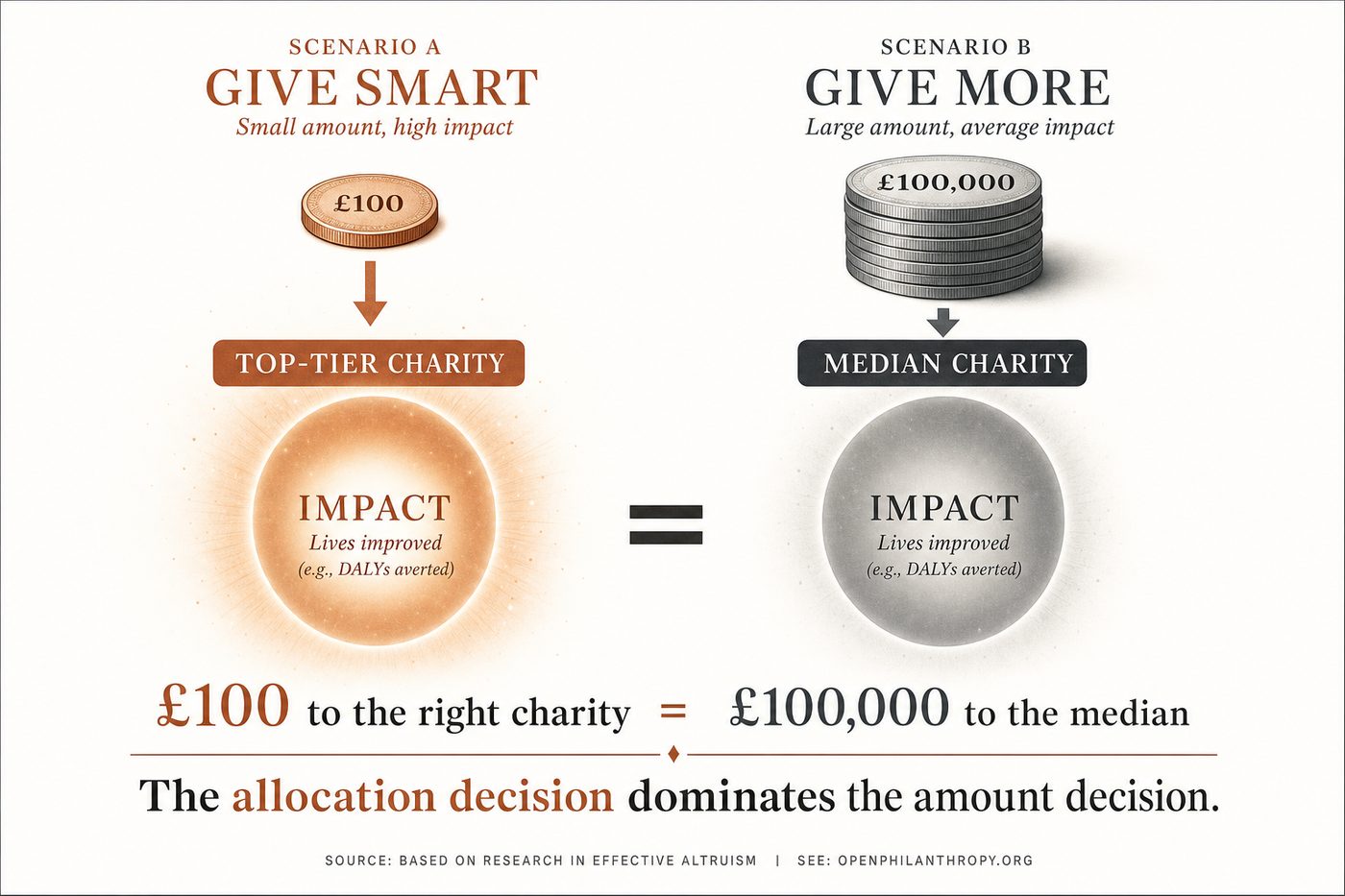
Choosing where matters more than choosing how much. If you're deciding between giving £100 to a cost-effective charity or £200 to a median one, the £100 gift likely produces more outcome. The allocation decision dominates the amount decision. This is counterintuitive for most people, who focus on the size of the donation.
You don't need to do the maths yourself. GiveWell, Founders Pledge, and the DCP3 have done the cost-effectiveness analysis. Your job as a donor is to trust-but-verify their methodology (it's published openly) and direct your giving accordingly. You don't need a spreadsheet. You need a shortlist.
Beware round-number anchoring. A charity that says "just £25 can save a life" is almost certainly overstating the cost-effectiveness or using a non-standard definition of "save." GiveWell's estimate of $3,000-$5,500 per life saved is based on rigorous modelling. If a claim sounds too good by comparison, it probably is.
Cost-effectiveness is not the only thing that matters. Some donors reasonably prioritise autonomy (GiveDirectly), systemic change (policy advocacy), or personal connection (local charities). The cost-per-outcome framework is the strongest tool for maximising health impact per dollar, but it's a framework, not a commandment. Knowing the numbers lets you make an informed tradeoff rather than an ignorant one.
The uncomfortable implication
If cost-effectiveness varies 100x across interventions, and most donors give without considering cost-effectiveness at all, then most charitable giving is dramatically less impactful than it could be. The Giving What We Can community estimates that the average dollar donated to a GiveWell top charity produces roughly 10-100x more health impact than the average dollar donated to a randomly chosen health charity.
That's not an argument for guilt. It's an argument for information. The gap exists because most people don't know it exists. Now you do.
One sentence
The most effective charities produce roughly 100x more impact per pound than the median. Knowing that number and acting on it is the single highest-leverage change most donors can make.
Sources
- The Moral Imperative Towards Cost-Effectiveness (Toby Ord, Giving What We Can) (accessed June 2026)
- How Much Does It Cost to Save a Life (GiveWell, February 2024 version) (accessed June 2026)
- Seasonal Malaria Chemoprevention | GiveWell (accessed June 2026)
- Insecticide-treated nets for preventing malaria (Cochrane review) (accessed June 2026)
- Oral rehydration therapy: a low-tech solution that has saved millions of lives (Our World in Data) (accessed June 2026)
- Cost-Effectiveness Analysis in Disease Control Priorities, Third Edition (DCP3) (accessed June 2026)
More in The Tally